


Why Work For Health Equity, not Equality? (free issue)
Equity and equality lead to different outcomes

Welcome! Thanks for stopping by. If you found your way here through a share or just by accident, you can subscribe for free and get your own issues!
Equality and equity. They come from the same Latin root, with equality from aequalitas and equity coming from aequitas. The words sound the same. But they don’t mean the same thing.
Equality means that everyone, you and I, are given the same resources. It could be that we receive the same bus ride to school, or the same medications for a chronic disease. But equity recognizes that everyone is different and has different circumstances. So we may need a different means of transportation to get to school (perhaps an adapted vehicle for a wheelchair, for example), or different medications for our illness for us both to thrive and reach our goals.
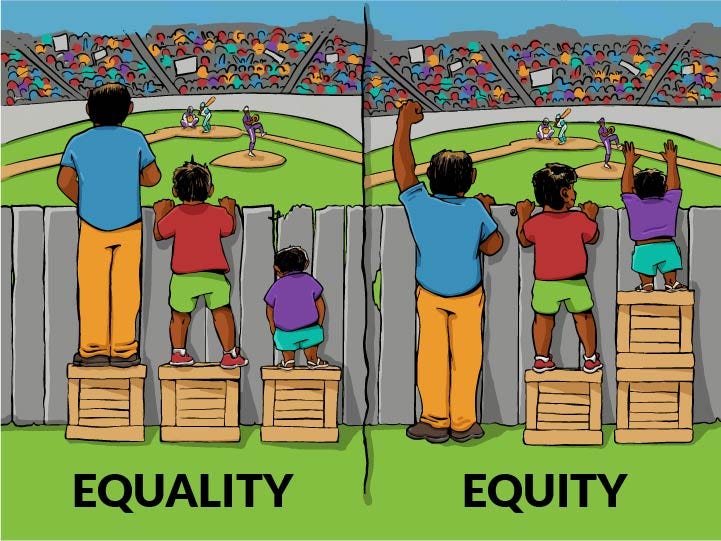
For some, when they hear the words equality and equity, there’s a knee-jerk reaction to the idea that someone is being given an unfair advantage. But this couldn’t be farther from the truth. By providing equity, we make things fair for everyone.
Health equity is essential
Health equity is vital for a healthy and productive population. Unfortunately, it’s not that way and, as I wrote in this blog post for Decipher Your Health, even your zip code can affect your health. I also address the issue in this post about black maternal health.
Equity affects children too, of course. According to Nationwide Children’s, “…healthy Black children are more likely to die after surgery than apparently healthy white children. In Ohio, Black babies die at more than twice the rate of white babies.”

Health equity doesn’t provide unfair advantages to anyone – it levels the playing field so everyone has equal opportunities, regardless of socioeconomics, age, health status, education, race, and gender.
Skin color affects health care
Many may deny it, but it’s true. The color of someone’s skin can affect how they are treated in the healthcare system. Take a quick look through any medical book. How many images of people with black skin do you think you will see? Very few, if any. In fact, according to a study published in 2018, a review of the most commonly used medical books showed there were only 4.5% of body images representing dark skin, despite 20.4% of the U.S. population being Black and 17% being a Person of Color.
How many images of people with black skin do you think you will see?
How does this make a difference – after all, isn’t an injury or a disease the same no matter what your skin color? That is where the mistakes come in.
How many times have you read something about a condition that says, “increasing redness on the skin” or “flushing of the skin.” Some skin doesn’t turn red – it goes darker or the skin tone changes. But it doesn’t turn red.
Or, how about taking oxygen readings using oximeters, those small devices that you put on the end of your finger to check to see how much oxygen is circulating in your body. Many people bought one when the COVID-19 crisis hit so they could monitor themselves at home.
I remember when these machines became readily available and we ended up doing routine oxygen levels on many patients, just like temperature and blood pressure. But what we didn’t know is that we (and you) shouldn’t rely completely on this device when used on people of color. Why? Because oximeters are “…three times more likely to give misleading readings among African-American patients.”
Equity here would mean that healthcare professionals learn about the aspects of medicine that affect people of different races in different ways, making adjustments to address these issues.
Education matters too
While doing my research, I wasn’t surprised to learn that people without a high school education were more likely to have type 2 diabetes than college graduates – almost twice as many. But what shouldn’t have surprised me was that people who did not complete high school had a life expectancy of 9 years shorter than college graduates overall.

People who don’t complete high school may be unable to educate themselves on their own and might not have a good understanding of health issues, how to follow treatments, and how to seek help if needed. They may be unable to find work that can pay health insurance or earn enough to buy healthy food. They may not understand what their healthcare professionals are saying when they do see them, and not feel confident enough to ask for more help.
…people who did not complete high school had a life expectancy of 9 years shorter than college graduates overall.
Equity here would ensure that people with lower education levels have access to information that they can understand in whatever method works for them. Also, equity would mean that healthcare professionals realize that they need to adapt their approaches when providing care.
Location affects equity
Where you live affects how well you can access health resources. Rural hospitals are closing. If you have to drive hours for healthcare, you have to have the time to go. You have to have the transportation. If you have children or family members you care for, you need resources to help you while you’re away.
But the problem isn’t only in rural areas. Big cities have healthcare deserts, parts of the cities where doctors don’t want to practice, so there is little access to medical appointments. One can argue that there are doctors in other parts of the city and this is true. But the patients have to be able to get there. Public transit isn’t always a viable option, many people don’t have cars. The time it takes to go out to further areas, again, is a factor. It is much harder to get to the appointments than it would be if there was something closer.
Equity in this situation would be to ensure that healthcare is locally available or other arrangements are available, such as consistent and reliable telehealth options.

Changing things so everyone has the access and care they need may not be easy or quick. But we have to stop kidding ourselves that the medical system serves everyone equally. It doesn’t. So, what can we do now to at least start making changes?
Leave your comment below and let’s get a conversation going.
This issue has a voiceover option for paid subscribers. It’s an added bonus for people who prefer to listen. To get the audio versions and extra issues, subscribe for only $5/month or $50/year. If you are a free subscriber and use computer-generated reading to listen due to visual impairment, please send me a message and I’ll arrange for you to get audio versions as well.